
ผลต่างระหว่างรุ่นของ "ปากแหว่งเพดานโหว่"
ไม่มีความย่อการแก้ไข |
ล เก็บกวาดทันใจด้วยสจห. |
||
| บรรทัด 56: | บรรทัด 56: | ||
<center> |
<center> |
||
<gallery> |
<gallery> |
||
ไฟล์:Cleftpalate3.png|Incomplete cleft palate |
|||
ไฟล์:Cleftpalate1.png|Unilateral complete lip and palate |
|||
ไฟล์:Cleftpalate2.png|Bilateral complete lip and palate |
|||
</gallery> |
</gallery> |
||
</center> |
</center> |
||
A direct result of an open connection between the [[oral cavity]] and [[nasal cavity]] is '''velopharyngeal insufficiency''' ([[velopharyngeal inadequacy|VPI]]). Because of the gap, air leaks into the nasal cavity resulting in a hypernasal [[voice]] [[resonance]] and nasal emissions.<ref name="Sloan">{{cite journal |author=Sloan GM |title=Posterior pharyngeal flap and sphincter pharyngoplasty: the state of the art |journal=Cleft Palate Craniofac. J. |volume=37 |issue=2 |pages=112–22 |year=2000 |pmid=10749049 |doi=10.1597/1545-1569(2000)037<0112:PPFASP>2.3.CO;2}}</ref> Secondary effects of VPI include speech [[articulation]] errors (e.g., [[distortions]], substitutions, and omissions) and compensatory misarticulations (e.g., [[glottal stop]]s and posterior nasal [[fricative]]s).<ref>Hill, J.S. (2001). Velopharyngeal insufficiency: An update on diagnostic and surgical techniques. Current Opinion in Otolaryngology and Head and Neck Surgery, 9, 365-368.</ref>. Possible treatment options include [[speech therapy]], prosthetics, augmentation of the posterior pharyngeal wall, lengthening of the palate, and [[Pharyngeal flap surgery|surgical procedures]].<ref name="Sloan" /> |
A direct result of an open connection between the [[oral cavity]] and [[nasal cavity]] is '''velopharyngeal insufficiency''' ([[velopharyngeal inadequacy|VPI]]). Because of the gap, air leaks into the nasal cavity resulting in a hypernasal [[voice]] [[resonance]] and nasal emissions.<ref name="Sloan">{{cite journal |author=Sloan GM |title=Posterior pharyngeal flap and sphincter pharyngoplasty: the state of the art |journal=Cleft Palate Craniofac. J. |volume=37 |issue=2 |pages=112–22 |year=2000 |pmid=10749049 |doi=10.1597/1545-1569 (2000) 037<0112:PPFASP>2.3.CO;2}}</ref> Secondary effects of VPI include speech [[articulation]] errors (e.g., [[distortions]], substitutions, and omissions) and compensatory misarticulations (e.g., [[glottal stop]]s and posterior nasal [[fricative]]s).<ref>Hill, J.S. (2001). Velopharyngeal insufficiency: An update on diagnostic and surgical techniques. Current Opinion in Otolaryngology and Head and Neck Surgery, 9, 365-368.</ref>. Possible treatment options include [[speech therapy]], prosthetics, augmentation of the posterior pharyngeal wall, lengthening of the palate, and [[Pharyngeal flap surgery|surgical procedures]].<ref name="Sloan" /> |
||
'''Submucous cleft palate''' (SMCP) can also occur, which is an occult cleft of the soft palate with a classic clinical triad of bifid uvula, notching of the hard palate, and zona pellucida. |
'''Submucous cleft palate''' (SMCP) can also occur, which is an occult cleft of the soft palate with a classic clinical triad of bifid uvula, notching of the hard palate, and zona pellucida. |
||
รุ่นแก้ไขเมื่อ 01:30, 24 มีนาคม 2552
| ปากแหว่งเพดานโหว่ (Cleft lip and palate) | |
|---|---|
 | |
| บัญชีจำแนกและลิงก์ไปภายนอก | |
| ICD-10 | Q35-Q37 |
| ICD-9 | 749 |
| DiseasesDB | 29604 29414 |
| eMedicine | ped/2679 |
ปากแหว่ง (อังกฤษ: cleft lip; ละติน: cheiloschisis) และเพดานโหว่ (อังกฤษ: cleft palate; ละติน: palatoschisis) หรือมักเรียกรวมกันว่าปากแหว่งเพดานโหว่ เป็นความผิดปกติแต่กำเนิดของการเจริญของใบหน้าระหว่างการตั้งครรภ์ การรักษาผู้ป่วยที่พิการปากแหว่งเพดานโหว่ทำโดยการผ่าตัดทันทีหลังคลอด อัตราผู้ป่วยปากแหว่งเพดานโหว่เกิดราว 1 ในทารกแรกเกิด 600-800 คน
ปากแหว่ง
ถ้ารอยแยกนั้นไม่ถึงส่วนเพดานปาก จะเรียกความผิดปกตินี้ว่า ปากแหว่ง หากเกิดที่ด้านบนของริมฝีปากในลักษณะช่องว่างเล็กๆ หรือเว้าเล็กน้อยเรียกว่า ปากแหว่งไม่สมบูรณ์ หรือปากแหว่งบางส่วน (partial or incomplete cleft) แต่หากรอยแยกนี้ต่อเนื่องไปถึงจมูกเรียกว่า ปากแหว่งสมบูรณ์ (complete cleft) ปากแหว่งอาจเกิดข้างเดียวหรือสองข้างก็ได้ ปากแหว่งมีสาเหตุจากการเชื่อมของขากรรไกรบนและส่วนยื่นจมูกด้านใกล้กลาง (medial nasal processes) เพื่อเป็นเพดานปากปฐมภูมิ (primary palate) ไม่สมบูรณ์
-
 ปากแหว่งข้างเดียวไม่สมบูรณ์ (Unilateral incomplete)
ปากแหว่งข้างเดียวไม่สมบูรณ์ (Unilateral incomplete) -
 ปากแหว่งข้างเดียวสมบูรณ์ (Unilateral complete)
ปากแหว่งข้างเดียวสมบูรณ์ (Unilateral complete) -
 ปากแหว่งสองข้างสมบูรณ์ (Bilateral complete)
ปากแหว่งสองข้างสมบูรณ์ (Bilateral complete)



ปากแหว่งรูปแบบหนึ่งเรียกว่า microform cleft ซึ่งมีความรุนแรงน้อยกว่า มีลักษณะเป็นรอยเล็กๆ บนริมฝีปากหรือมีลักษณะคล้ายแผลเป็นจากริมฝีปากไปยังจมูก ในบางรายกล้ามเนื้อหูรูดปากใต้แผลเป็นนั้นอาจผิดปกติซึ่งต้องได้รับการผ่าตัด ทารกที่เกิดมามีความผิดปกติดังกล่าวจำเป็นต้องได้รับการประเมินความรุนแรงจากแพทย์ด้านใบหน้าและปากทันที
-
 เด็กชายอายุ 3 เดือนปากแหว่งข้างเดียวไม่สมบูรณ์ ก่อนได้รับการผ่าตัด
เด็กชายอายุ 3 เดือนปากแหว่งข้างเดียวไม่สมบูรณ์ ก่อนได้รับการผ่าตัด -
 เด็กชายคนเดียวกัน 1 เดือนหลังจากผ่าตัด
เด็กชายคนเดียวกัน 1 เดือนหลังจากผ่าตัด -
 เด็กชายคนเดียวกันอายุ 1 ปี 5 เดือน สังเกตว่าแผลเป็นจะดูจางลงตามอายุ
เด็กชายคนเดียวกันอายุ 1 ปี 5 เดือน สังเกตว่าแผลเป็นจะดูจางลงตามอายุ



-
 เด็กหญิงอายุ 6 เดือนปากแหว่งข้างเดียวสมบูรณ์ ก่อนได้รับการผ่าตัด
เด็กหญิงอายุ 6 เดือนปากแหว่งข้างเดียวสมบูรณ์ ก่อนได้รับการผ่าตัด -
 เด็กหญิงคนเดียวกัน 1 เดือนหลังจากผ่าตัด
เด็กหญิงคนเดียวกัน 1 เดือนหลังจากผ่าตัด -
 เด็กหญิงคนเดียวกัน อายุ 5 ปี 4 เดือน สังเกตว่าแผลเป็นจะดูจางลงตามอายุ
เด็กหญิงคนเดียวกัน อายุ 5 ปี 4 เดือน สังเกตว่าแผลเป็นจะดูจางลงตามอายุ


เพดานโหว่
เพดานโหว่ เป็นภาวะที่แผ่นกระดูกของกะโหลกศีรษะ 2 แผ่นไม่เชื่อมกันเป็นเพดานแข็ง อาจมีช่องโหว่ของเพดานอ่อนได้ด้วยเช่นกัน ผู้ป่วยส่วนมากมักมีปากแหว่งร่วมด้วย เพดานโหว่เกิดราว 1 ในทารกแรกเกิดมีชีพ 700 คนทั่วโลก[1]
Palate cleft can occur as complete (soft and hard palate, possibly including a gap in the jaw) or incomplete (a 'hole' in the roof of the mouth, usually as a cleft soft palate). When cleft palate occurs, the uvula is usually split. It occurs due to the failure of fusion of the lateral palatine processes, the nasal septum, and/or the median palatine processes (formation of the secondary palate).
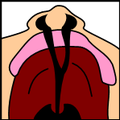
The hole in the roof of the mouth caused by a cleft connects the mouth directly to the nasal cavity.
Note: the next images show the roof of the mouth. The top shows the nose, the lips are colored pink. For clarity the images depict a toothless infant.
-
 Incomplete cleft palate
Incomplete cleft palate -
 Unilateral complete lip and palate
Unilateral complete lip and palate -
 Bilateral complete lip and palate
Bilateral complete lip and palate



A direct result of an open connection between the oral cavity and nasal cavity is velopharyngeal insufficiency (VPI). Because of the gap, air leaks into the nasal cavity resulting in a hypernasal voice resonance and nasal emissions.[2] Secondary effects of VPI include speech articulation errors (e.g., distortions, substitutions, and omissions) and compensatory misarticulations (e.g., glottal stops and posterior nasal fricatives).[3]. Possible treatment options include speech therapy, prosthetics, augmentation of the posterior pharyngeal wall, lengthening of the palate, and surgical procedures.[2]
Submucous cleft palate (SMCP) can also occur, which is an occult cleft of the soft palate with a classic clinical triad of bifid uvula, notching of the hard palate, and zona pellucida.
แหล่งข้อมูลอื่น
บทความแพทยศาสตร์นี้ยังเป็นโครง คุณสามารถช่วยวิกิพีเดียได้โดยการเพิ่มเติมข้อมูล |
- ↑ "Statistics by country for cleft palate". WrongDiagnosis.com. สืบค้นเมื่อ 2007-04-24.
- ↑ 2.0 2.1 Sloan GM (2000). "Posterior pharyngeal flap and sphincter pharyngoplasty: the state of the art". Cleft Palate Craniofac. J. 37 (2): 112–22. doi:10.1597/1545-1569 (2000) 037<0112:PPFASP>2.3.CO;2. PMID 10749049.
{{cite journal}}: ตรวจสอบค่า|doi=(help) - ↑ Hill, J.S. (2001). Velopharyngeal insufficiency: An update on diagnostic and surgical techniques. Current Opinion in Otolaryngology and Head and Neck Surgery, 9, 365-368.